










|
Getting your Trinity Audio player ready...
|
Covid-19 is a great leveler? Look again. On-the-ground reports show it is exacerbating pre-existing social inequalities
By JC Mercado
There is a growing body of evidence indicating that the impacts of today’s global scourge and that the measures states take to counter it disproportionately put at risk those who are socioeconomically disadvantaged. While these impacts are interlinked, poorer families are more likely to have pre-existing conditions like asthma and hold public-facing jobs than well-off ones. This unevenness in risks highlights yet a more pressing social inequality — health access.
Last month, a 53-year old man died at the doorsteps of a hospital in Bengaluru, India after being denied admission into 18 hospitals. Meanwhile, people of means in the same capital city in India’s southern Karnataka state can book a hotel room for mandatory quarantine at a cost of about 10,000 rupees ($132) a night. While this may seem an outlier, the rapid increase in Covid-19 infections in specific parts of the region may push it to a recurring reality.
Inaccessible basic healthcare
Health inequality remains one of the major obstacles to human development in Asia, with as much as 80 percent of the population living without access to affordable basic healthcare. Such divide among those who can and cannot pay is growing amid the pandemic as issues surrounding medical care range from underfunded government hospitals to the prohibitive costs of five-star quarantine hotels. In addition, the rising costs of medical care, be it specific to Covid-19 or not, especially in private hospitals in Asia, are setting off alarm bells for a rethinking of healthcare reforms in the region.
As the pandemic continues to ravage Asian countries differentially, it is well worth noting how the financing structures of healthcare systems impact the spread and fatality rates of the coronavirus, and, more importantly, those at the bottom rung.

Countries with higher healthcare spending per capita have mixed results in managing the Covid-19 pandemic
In Asia, countries with higher combined private and public health spending per capita (in US$) tend to have less Covid-19 deaths per million than those with smaller healthcare industries. But globally, richer countries with higher per capita healthcare spending tend to have mixed results. For example, the high-income European countries have higher mortality rates.
Hover the cursor over the graph to view more data.
[Data sources: Global Health Observatory, World Health Organization, 2020 and Johns Hopkins University, 2020]
More privatized healthcare systems tend to have higher Covid-19 cases and mortality rates
The privatization of healthcare systems is often equated with increasing efficiency and quality healthcare service. Yet countries like Vietnam and Thailand seem to belie this notion, because they are faring better than those with more privatized systems like India and the Philippines.
The private sector in the Asian healthcare industry was booming even before the pandemic, and had been projected to grow to $486.72 billion in 2019.
A preliminary study by the United Nations Development Programme (UNDP) found that a 10-percent increase in private health expenditure results in a 4.85-percent increase in Covid-19 cases. Worse, the same increase may also lead to 6.91-percent spike in Covid-19 deaths, according to another model in the same study.
This lends credence to experts’ findings that Vietnam’s huge public health spending and Thailand’s often-praised universal healthcare coverage may prove critical in managing coronavirus infection and fatality rate. One outlier, however, is Myanmar which has managed to keep both infections and deaths to a minimum despite a higher ratio of private healthcare spending. But the fact that 86 percent of its hospitals are run by the State, combined with the fast growth of both public and private healthcare expenditure [see Graph 4], may have helped this.
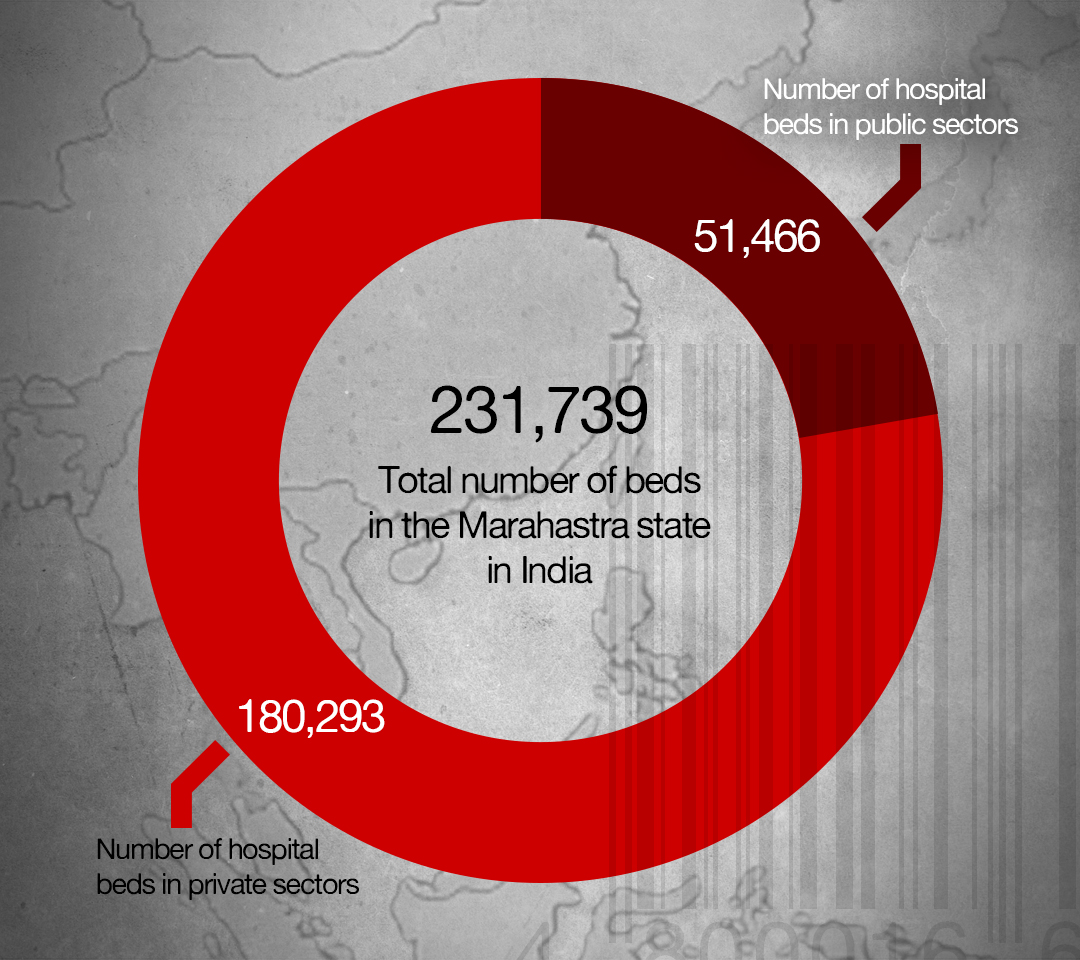
In addition, worse-off countries like India, which has now breached a million cases, also confirm this. Private hospitals own more than three times hospital beds, ICU beds, and ventilators than public hospitals in Maharashtra – now the worst-hit city in the world’s largest democracy. Afghanistan, which has the highest Covid-19 death rate, also has the highest private-to-public spending ratio in the region.
Hover the cursor over the graph to view more data.
[Healthcare spending in US$. Source: Global Health Observatory, World Health Organization, 2020]
Countries with higher public healthcare spending may be more prepared
Across the Asian region, high-income countries like Japan, China, and the Republic of Korea have the highest number of beds, physicians, and nurses per 10,000 population, followed by Maldives and Sri Lanka, which both have high public healthcare spending compared to private.
With the incidence of coronavirus infections rising in South Asia and in parts of Southeast Asia, hospital occupancy rates are starting to max out. With the exception of Maldives and Sri Lanka, South Asian countries tend to be underprepared for an outbreak, as seen in single-digit hospital beds and medical professionals per 10,000 population.
Countries like Singapore and Malaysia have a relatively higher number of physicians and nurses in the region but are low in hospital beds. This can, in part, be attributed to the rise in health tourism in these countries. Another outlier is the Philippines, which currently has 2.4 nurses per 10,000 population despite supplying 19,000 nurses globally based on its labor export policy.
Hover the cursor over the graph to view more data.
[Healthcare Capacity by Physicians, Nurses, and Hospital beds per 10,000 population. Source: Global Health Observatory, World Health Organization, 2020]
Note: Relative Capacity Score is computed by averaging percentage of country series relative to Japan’s (Japan = 100).
Growing private and public health spending in Asia
Both private and public healthcare spending per capita in Asia has generally been growing over the past few years except for Japan and Indonesia’s declining private sectors. Low- and middle-income countries like Myanmar, Lao PDR, and Pakistan are growing faster on average but others like India, Bangladesh, Malaysia, and the Philippines are lagging behind in both private and public healthcare spending. However, healthcare spending in major economies including China have dropped by at least 1% since the coronavirus outbreak, according to a recent study by the Economist Intelligence Unit.
Hover the cursor over the graph to view more data.
[Source: Global Health Observatory, World Health Organization, 2020
On the other hand, developing countries in the region like the Philippines are racking up debt to spend on hospital beds, isolation facilities, and remuneration adjustments for front liners.
Privatization exacerbates health inequality
As mentioned, the impacts of Covid-19 are uneven across country borders. Asia has one of the biggest pre-pandemic gaps in life expectancy by income deciles and health financing. A regression analysis of the UNDP’s Inequality in Life Expectancy Index and the ratio of private and public spending per capita of countries show this to be true. At least 42 percent of inequality in life expectancy may be tied to increased privatization in healthcare globally, as the following graph shows.
Hover the cursor over the graph to view more data.
Note: The private-to-public healthcare spending ratio was transformed using natural algorithm (ln-transformed) to minimize the effect of outliers and extreme values, accounting for high global inequality in healthcare expenditure per capita
Out-of-pocket spending was on the rise even before the pandemic
Out-of-pocket spending (OOPS) disproportionately burdens the poor and socioeconomically disadvantaged, and has been rising in the past few years. Estimates from World Bank data show a 36.13-percent average annual growth (2010-2017) in OOPS. Excluding rich countries, East and Asia Pacific’s OOPS grew at an annual average of 78.44 percent and South Asia’s by 60.65 percent in the same period. Myanmar, which has the highest annual growth rate in both public and private spending (Graph 4), also has the biggest jump in out-of-pocket in capita expenditure.
Hover the cursor over the graph to view more data.
Source: Global Health Observatory, World Health Organization, 2020
The poor in India, Bangladesh, and Nepal will be most impacted by rising health inequality
To illustrate these devastating consequences further, at least one in six poor households in the three countries mentioned above, or almost 60 million people, were already spending at least a tenth of their income on out-of-pocket healthcare expenditure before the pandemic. In Bangladesh alone, at least one in five poor households were spending 10 percent of their income on doctor visits before the pandemic.
Hover the cursor over the graph to view more data.
Source: Global Health Observatory, World Health Organization, 2020
A cause and consequence of inequality
Being stratified by the capacity to pay for healthcare is both a cause and consequence of inequality. Such disparities among and within countries in Asia are more worrisome now as people grapple with Covid-19 and the costs of its treatment. In India, for example, while most people have primary healthcare coverage in public hospitals, private hospitals represent 60 percent of beds, 60 percent of in-patients, and 80 percent of doctors.
As public hospitals in major cities now feature dayslong queues, this divide between the rich and the poor is bound to grow further. While countries like Myanmar have significantly benefited from its higher share of public spending, this might not last if the growth in out-of-pocket spending continue to outpace government investments on its citizens’ healthcare.
Amid this global health crisis, the most vulnerable in society bear the brunt of its aftermath. It’s estimated that at least 1.6 billion people, mostly informal workers, will have lost their jobs in the coming months, putting millions more into extreme poverty. The combined loss of income and rising costs of healthcare will further stoke health inequality – and the poor will be reeling from its impact.●
JC Mercado has more than 10 years of data research and content writing experience. He is also a long-time peasant advocate and food sovereignty activist in the Philippines. He writes about human rights and rural people’s welfare in the Philippines and in Asia. Catch him on Twitter as @darnitjc.







{kind=link}